Important Dermatology Questions For NEET PG/FMGE
Dec 19, 2024

Q.1 A 38-year-old male presents with complaints of 4 hypopigmented, hypoesthetic, and dry lesions distributed over his back accompanied by a gradual loss of sensation in the affected areas over the past few months. Examination findings are shown in the image below. What is the most likely diagnosis for this patient?

- Borderline Lepromatous
- Borderline Tuberculoid
- Lepromatous
- Tuberculoid
Answer: 2) Borderline Tubercuoid
Explanation:
A) Borderline tuberculoid
- Borderline Tuberculoid leprosy typically presents with a few hypopigmented skin lesions that are well-demarcated and accompanied by hypoesthesia due to nerve involvement and satellite lesions may be seen (Arrowmark in the image).
- The Ridley-Jopling classification is a system for classifying different types of leprosy based on clinical, histopathological, and immunological features.
- It was developed in 1966 by David M. Ridley and John H. Jopling.
- Indeterminate type and pure neuritic type are not included in the Ridley-Jopling classification.
Also read: Important One-liner in Dermatology
Q.2 As a pathologist in a prestigious private clinic, a physician contacts you for urgent feedback on a skin biopsy from a prominent politician. Suspecting psoriasis, what histopathological findings in the stratum corneum would you communicate to the attending physician?
- Hyperkeratosis, parakeratosis, and microabscesses
- Kogoj’s spongiform pustules
- Camel foot appearance
- Suprapapillary thinning
Answer: 1) Hyperkeratosis, parakeratosis, and microabscesses
Explanation:
The various histopathological findings in the different skin layers seen in a patient with psoriasis are as follows:.
| Layer | Findings | Image |
| Stratum Corneum | - Hyperkeratosis (increased thickening of stratum corneum) - Parakeratosis (retention of nuclei in stratum corneum) - Munro's microabscess (collection of neutrophils) | 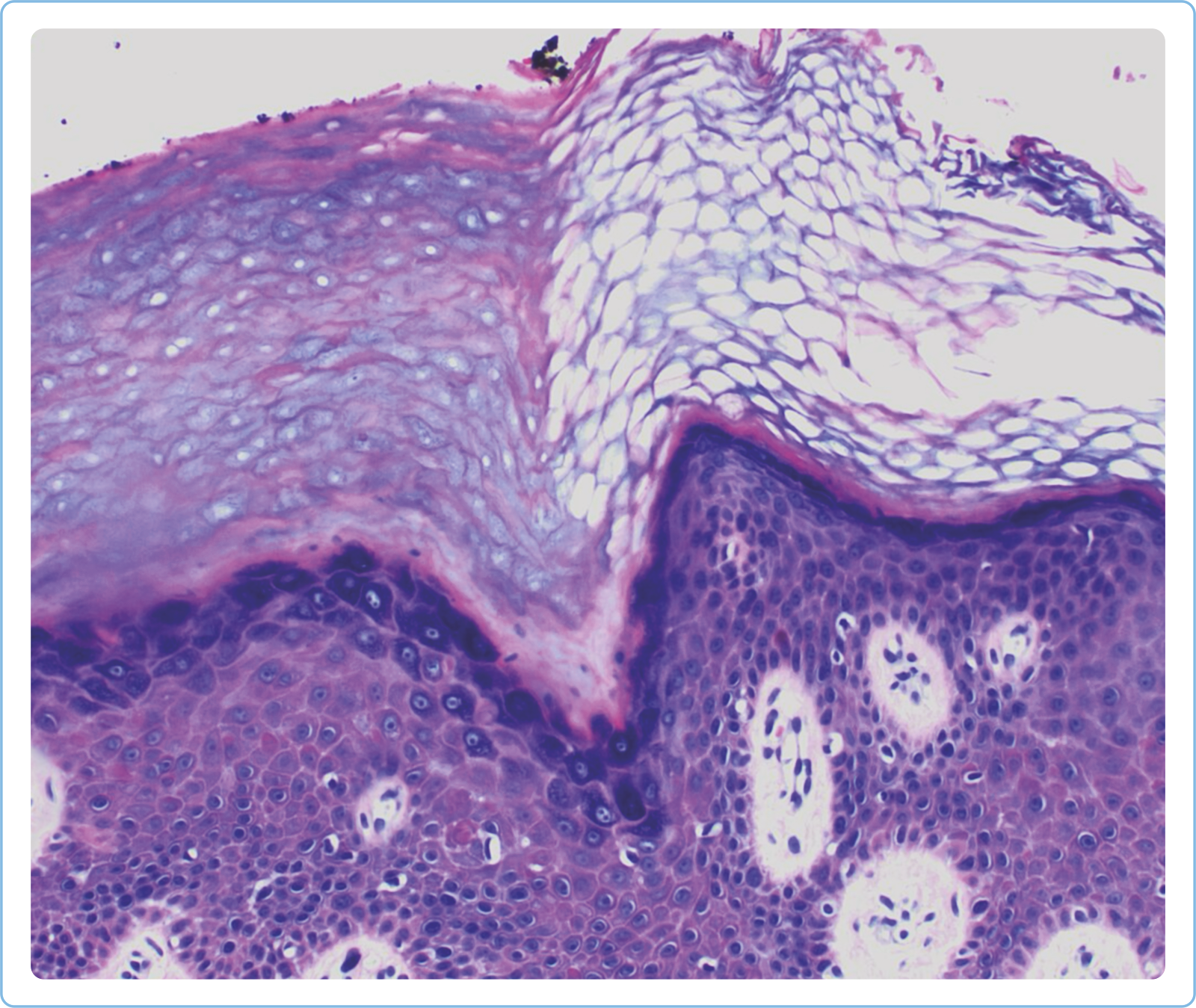 |
| Stratum Granulosum | - Agranulocytosis/ Agranulosis (absent granular layer) | Same as above |
| Malpighian layer (Stratum) Spinosum and Basale) | - Acanthosis (increased thickness) of stratum spinosum - Kogoj's Spongiform pustules (collection of neutrophils) | Same as above |
| Rete ridges | - They are elongated and club-shaped (Camel foot appearance). | 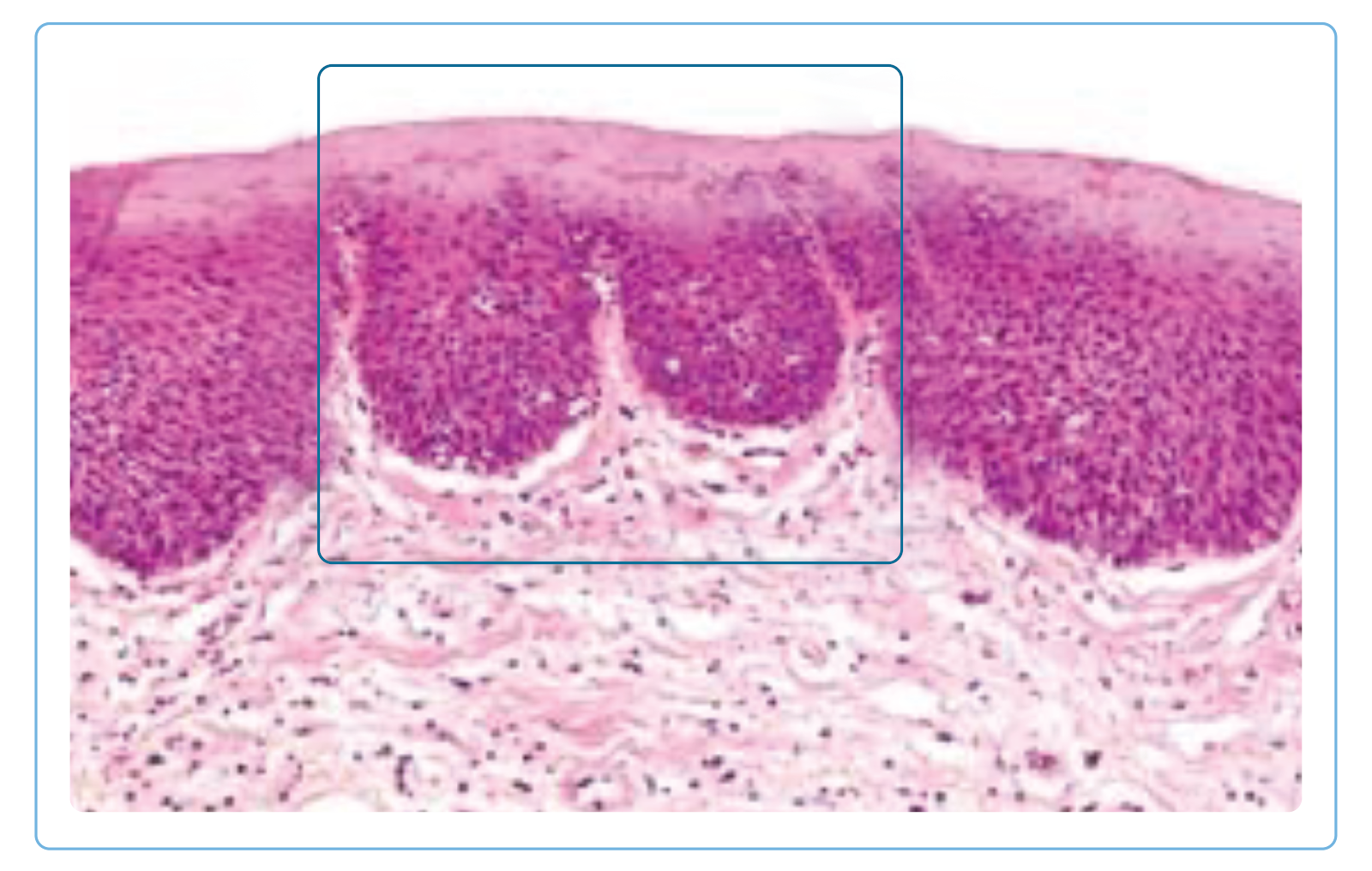 |
| Dermis | - Suprapapillary thinning is seen, the first histopathological sign. - Dilated tortuous blood vessels- Inflammation | 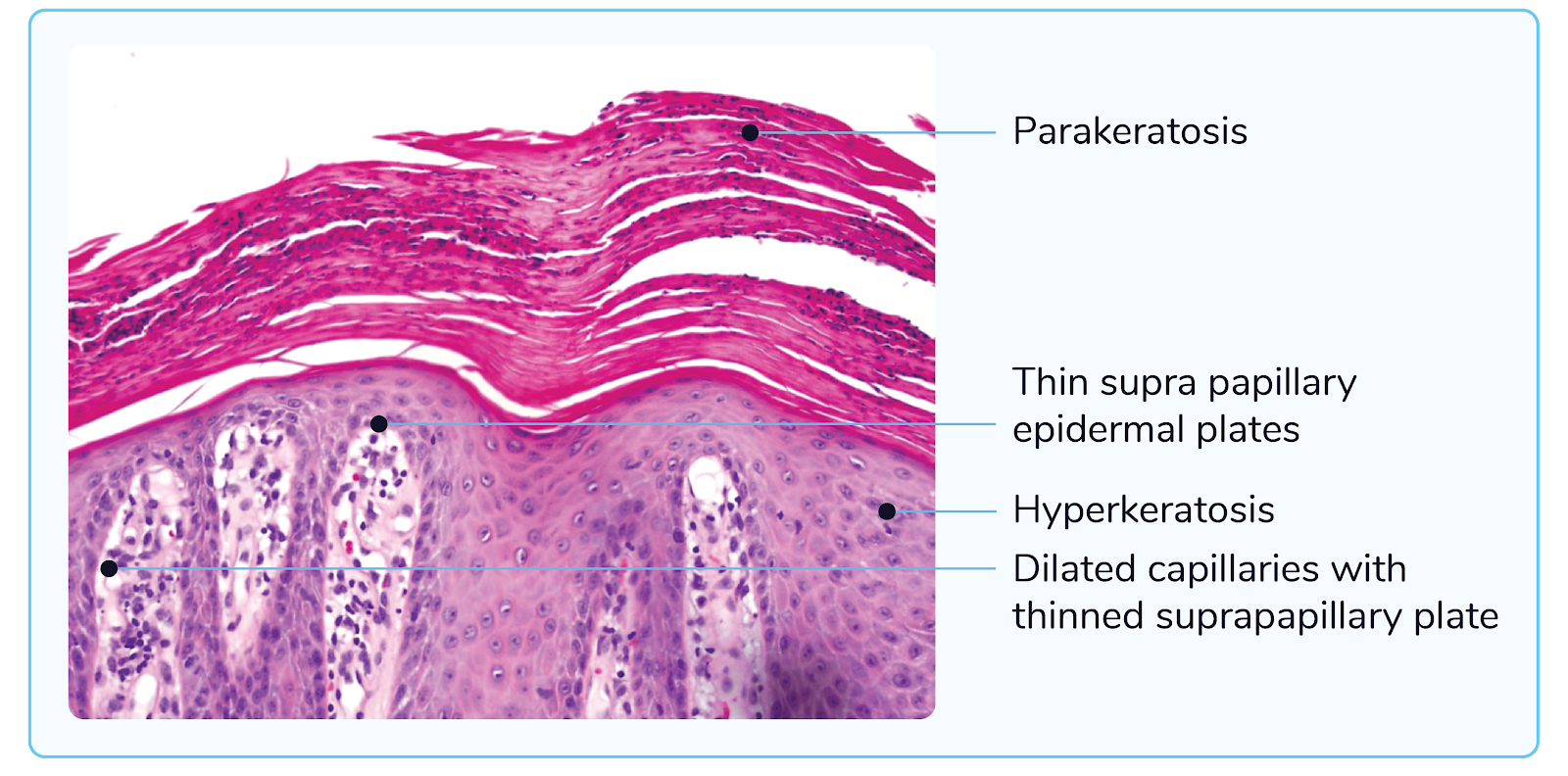 |
Q.3 At your community medicine posting, a farmer arrives complaining of multiple nodules over his right leg after being pricked by a thistle. Examination findings are given in the image below:

What would you expect to find on a microscopic examination of tissue from one of his lesions?
- Asteroid bodies
- Black Granules
- Muriform bodies
- Spherules containing endospores
Answer: 1) Asteroid Bodies
Explanation:
The patient’s presentation, along with the linear distribution of nodules, is suggestive of sporotrichosis/Rose Gardner’s disease caused by Sporothrix schenckii.
Sporotrichosis:
- Subcutaneous fungal infection that typically occurs after the fungus is traumatically inoculated into the skin, often through thorn pricks, splinters, or scratches from contaminated plant material.
- Enzymes secreted by fungus, such as serine & aspartate proteinases, help in local invasion.
- Sporothrix schenckii has a tendency to spread along lymphatics.
- Clinical manifestations:
- Incubation period: 3 weeks.
- Types:
| Lympho-cutaneous | - M/C type (80%) - Painless modulo-ulcerative lesions along the lymphatics. - Lymph nodes can become enlarged, suppurative, & indurated and have a cord-like feeling on palpation. |
| Osteoarticular | Seen in alcoholics. |
| Pulmonary | Can be seen in underlying COPD. |
| Disseminated | Seen in immunocompromised patients. |
| Fixed cutaneous | Single nodule, less progressive & not spread by lymphatics. |
- Risk factors: walking barefoot, farmers & gardeners.
- Laboratory diagnosis:
- KOH mount: elongated yeast cells of 3-5 ?m in diameter (low sensitivity).
- Histopathological staining with methenamine silver: Cigar-shaped asteroid bodies
- Consists of a central basophilic yeast cell surrounded by radiating extensions of eosinophilic mass, composed of antigen-antibody complexes.
- Such eosinophilic halo is described as the Splendore Hoeppli phenomenon.
- Culture is the most definitive test for diagnosis.
The image below shows the culture of S. schenckii:


The image below shows the asteroid body and Splendour Hoeppli phenomenon:

- Treatment:
- DOC for all forms of Sporotrichosis: Itraconazole (except disseminated form; DOC is amphotericin-B).
- Treatment is given for 2-4 weeks after the lesions resolve
Also read: Bacterial Infections in Dermatology: Overview and Management
Q.4 A 65-year-old female came with complaints of a painless nodule on the right palm for the past 3 weeks. She gave a history of sustaining a thorn prick injury to the palm 4 weeks ago. On examination, the lesions appear as shown below. What is the most likely diagnosis?
- Keratoacanthoma
- Bowens disease
- Mycosis fungoides
- Actinic keratosis

Answer: 1) Keratoacanthoma
Explanation:
Option 1: The given image showing an exophytic nodule with the central keratinous debris is suggestive of Keratoacanthoma.
Keratoacanthoma is a low-grade squamous cell cancer. It presents as a proliferating dome-shaped keratin-filled crater. Patients usually give a prior history of minor trauma.
M/C Site: Face > hands
Phases of growth:
Growth, Maturation, and resolution phase
- It starts as a papule.
- Develops into a dome-shaped nodule with a central keratin plug.
- Outer epidermal lining extends to surrounding skin
- Plug falls off.
- Lesion disappears.
The treatment of choice is an excisional procedure with 4mm margins.
Also Read: Modes of Ventilation: Types and Uses
Q.5 A 28-year-old male presents to the STD clinic with a history of swelling in the inguinal region, as shown in the image below. He has a history of unprotected sexual intercourse in the past few months and reports a painless ulcer, which healed without scarring. Which of the following is false regarding this condition? 

- Caused by Chlamydia trachomatis L1-L3
- Can be associated with hepatitis C co-infection
- Presents with an indurated ulcer and painless lymphadenopathy
- Esthiomene is a complication in the tertiary stage of this disease
Answer: 3) Presents with an indurated ulcer and painless lymphadenopathy
Explanation:
The given clinical presentation of a male with a history of unprotected sexual intercourse, swelling in the inguinal region (inguinal lymphadenopathy), and a painless ulcer that has healed without scarring is suggestive of lymphogranuloma venerum, caused by Chlamydia trachomatis. The incorrect statement is that it presents with an indurated ulcer and painless lymphadenopathy.
Also read: Viral Skin Infections
Hope you found this blog helpful for your best NEET PG Coaching online. For more informative and interesting posts like these, keep reading PrepLadder’s blogs.
Download PrepLadder's best app for neet pg preparation for Android
Download PrepLadder's best app for neet pg preparation for ios

PrepLadder Medical
Get access to all the essential resources required to ace your medical exam Preparation. Stay updated with the latest news and developments in the medical exam, improve your Medical Exam preparation, and turn your dreams into a reality!
Top searching words
The most popular search terms used by aspirants
- NEET PG Dermatology
- NEET PG Dermatology Preparation
PrepLadder Version X for NEET PG
Avail 24-Hr Free Trial