Tumours of The Parapharyngeal Space
Aug 15, 2024

Introduction
PPS tumors account for 0.5% of all head and neck tumors. They are quite uncommon. Most common: 45% - salivary gland tumor origin arising in the pre-styloid compartment. Around 75% of tumors are benign in nature, and out of these tumors, 64% are pleomorphic adenomas. Adenoid cystic carcinomas and muco-epidermoid carcinomas are the frequently reported malignancies. 41% - neurogenic lesions are present in the PPS, mostly benign. Out of these, 52% are paragangliomas, 27% are schwannomas, and 9% are neurofibromas.
Types of tumors of PPS
|
Benign Tumors |
Malignant Tumors |
||
|
Name |
Frequency |
Name |
Frequency |
|
Pleomorphic adenoma Carotid paraganglioma Vagal paraganglioma Schwannoma Other benign salivary tumors Other tumors Meningioma Neurofibroma |
34 17 16 11 8 5 2 3 |
Adenoid cystic carcinoma Mucoepidermoid carcinoma Other malignant salivary tumors Lymphoma Carotid body paraganglioma Vagal paraganglioma Other malignant tumors |
5 3 4 2 1 1 2 |
Deep-lobe parotid neoplasms are common in the pre-styloid compartment, while paragangliomas or schwannomas are present in the post-styloid compartment. The majority of these are benign in nature.
Salivary Gland tumors
These are the most common tumors of PPS. They are invariably found in the prestyloid compartment and arise from the deep lobe of the parotid gland. A minority of these tumors can also arise from the extra-parotid salivary glands in the PPS. These tumors are histologically characterized as pleomorphic adenomas. In rare cases, Warthin’s tumor, oncocytoma, and benign lymphoepithelial lesion can also be seen.
In rare cases of malignancy, salivary carcinomas can arise, including mucoepidermoid carcinoma, malignant mixed tumors, adenoid cystic carcinoma, and adenocarcinoma.
Neurogenic Tumors
Neurogenic Tumors are commonly occurring in the post-styloid compartment of the para-pharyngeal space, these involve Paraganglioma, Schwannoma and Neurofibroma.
Other types of tumors are extremely rare.

Paraganglioma
Paragangliomas are cells arising from the carotid bodies. These arise from paraganglionic cells, a component of the sympathetic nervous system. The paraganglionic cells are sensitive to fluctuations of blood gas partial pressure, especially carbon dioxide, but they are also responsive to oxygen and pH fluctuations.
Paraganglionic cells are positive for neuron-specific enolase (have a neuroectodermal tissue origin). High metabolic rate is related relatively to common neoplastic variation in such a small body of cells. These tumors have the highest blood flow compared to any organ relative to their size. These are associated with multiple endocrine neoplastic (MEN) syndrome.
Most of these tumors appear as asymptomatic neck or intraoral mass (rarely) by means of medial displacement of the superior pole of the palatine tonsil, a unilateral bulge of the tonsil is noticeable.
As a rule of thumb, there are two differential diagnoses of a unilateral bulge of the tonsils, which include.
- This bulge could be indicative of either a peritonsillar abscess or a PPS lesion.
- The peritonsillar lesion will have no neck swelling but there will be swelling in the PPS lesion.
- This swelling will occur because of the extension of PPS to hyoid bone. On the contrary, peritonsillar space is the space between the capsule of the tonsil and the superior constrictor muscle.
Parapharyngeal lesions are detected incidentally in magnetic resonance imaging (MRI) and computed tomography. Around 10% of paragangliomas are multicentric. Thus, whole-body MRI should be performed to examine sites such as the aortic arch and adrenal sites. Nearly 3% of paragangliomas are secretory, i.e., these tumors can secrete hormones such as norepinephrine, epinephrine, and dopamine, or catecholamines, and present with systemic symptoms.
Patients should be screened for catecholamine release, even if they have no symptoms. Tests such as Serum levels of catecholamines and their by-products, such as vanillyl mandelic Acid and urinary metanephrines, can be performed.
Characteristic imaging findings on MRI will show salt and pepper appearance and LYRE sign - splaying of the internal and external carotid arteries. At the gross examination - paragangliomas are brownish in appearance and are well encapsulated.
Benign and malignant paraganglioma will be difficult to differentiate without histopathological examination. On the basis of histopathology, paragangliomas demonstrate a clustering of epithelioid chief cells and sustentacular cells in an extremely vascular and fibrous stroma, forming a specific pattern known as the Zellballen pattern.
Vagal Paragangliomas
These originate from the vagus nerve and are rare tumors of neural crest origin. So, neuron-specific enolase will be positive in this case. Vagal paragangliomas are extremely slow-growing and are also encapsulated. It is known to occur at the base of the skull, where the vagus nerve and the 9th-10th nerves are located. These tumors mostly arise in the nodose ganglion, the inferior ganglion in the vagus nerve. It can occur at any part of the vagus nerve and its branches. It usually involves the jugular foramen.
These tumors present in patients aged between 30-70 years. Around half of the tumors arise from the vagus nerve or the sympathetic trunk. The lesion can arise juxtaposed to the jugular bulb, leading to the involvement of the temporal bone.
A large jugular bulb paraganglioma (glomus jugulare) is indistinguishable from nodose ganglion paraganglioma. Catecholamine secretion is common in both types of tumors.
Malignant Paraganglioma
Upto 10% of paragangliomas are of a malignant nature. The benign and malignant tumors are indistinguishable solely on the basis of histopathological features alone if the tumors have not metastasized (either regionally or to distant organs).
Surgeons can diagnose malignant paragangliomas based on evidence of clinical invasion and aggressive behavior. Since these malignant lesions cannot be completely removed, post-operative radiotherapy is mandatory.
To read more about Familial and multiple paragangliomas & phaeochromocytomas, MEN syndrome, Schwannoma, Neurofibroma, von Recklinghausen’s disease, rare Tumors of PPS, metastasis to the parapharyngeal space and the spread within the tumor within the parapharyngeal space, sign up to the prepladdder app. The residency ENT discusses these topics in detail.
Clinical Features of the Parapharyngeal Space Tumours
- These tumors are clinically present as neck swelling, although peritonsillar space lesions present as bulges of the tonsils.
- Clinical features include:
- Oropharyngeal mass
- Nasal obstruction
- Eustachian tube obstruction
- Dysphagia, because the posteropharyngeal wall will have indentation occurring as a result of medial displacement of the tonsil.
- Dyspnea due to narrowed oropharynx.
- Dysphonia
- Obstructive sleep apnea
- Cranial nerve deficits
- Horner’s syndrome
- Trismus
- Symptoms of catecholamine excess
- Headache
- Palpitation
- Excessive perspiration
- Hypertension, Orthostatic changes in blood pressure
- Nausea
- Pallor
- Syndrome of inappropriate antidiuretic hormone secretion (SIADH) or Schwartz-Bartter Syndrome
- Squamous cell carcinomas
- Neuroblastomas
- Small-cell neuroendocrine carcinomas
- Adenoid cystic carcinomas
- Undifferentiated carcinomas and sarcomas
Diagnosis of the Parapharyngeal Space Tumors
Imaging:
- A radiological examination is required to evaluate a patient with a suspected PPS mass and should be performed prior to the biopsy.
- As a second diagnostic measure, computed tomography (CT) or ultrasound-guided fine needle aspiration cytology can be performed afterward.
- On the basis of the results from these two diagnostic tests, a specific plan of action is to be determined.
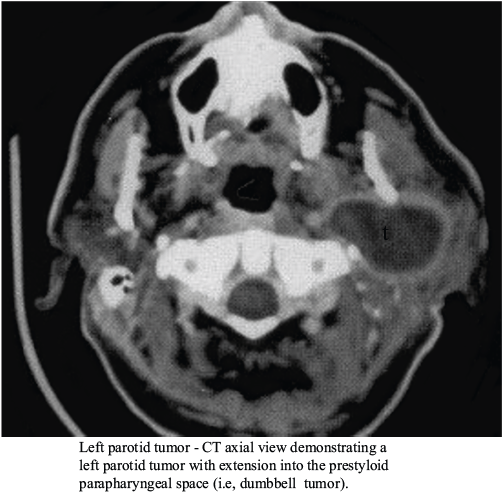
Computer Tomography Scan (CT)
- A CT scan can help localize the PPS mass to either the pre- or post-styloid space.
- It can demonstrate the tumor's origin and whether it occurred in the deep lobe of the parotid.
- It can also help position the tumor in the extra parotid region by showing whether the fat plane between the parotid and the mass is preserved.
- This measure is superior to an MRI examination in demonstrating the presence of calcifications with the tumor and the involvement of bony structures.
- Using the contrast infusion mode, the relationship of the mass to the greater vessels, especially the internal carotid artery and internal jugular vein, may be appreciated, although enhanced post-styloid lesions may be difficult to separate from the carotid artery.
- It is widely used because of lower costs and easy availability, although concerns about radiological exposure remain.
Magnetic Resonance Imaging
- An MRI aids in differentiating between the tumor and muscle, offering greater resolution in defining the great vessels and their relationship to the tumor.
- The intracranial extension is better delineated on MRI.
- Disadvantages: higher costs and longer time, and it can also be a hindrance to performing it in claustrophobic people.
- Some patients may have implants or pacemakers, which are incompatible with an MRI.
- It has a poor ability to determine the involvement of the bone.
- The left side shows the MRI scan of the tumor involving the deep lobe of the parotid (only partial involvement of the parotic is there), and such tumors are accessible from the oropharynx.
- The MRI scan will depict a salt-and-pepper appearance with dark grey and light grey areas.
- A T2-weighted image will show a hyperintense lesion.
Angiography
- Angiography is recommended to diagnose vascular lesions and in cases of suspected malignancy.
- It can demonstrate the relationship between poststyloid lesions to the great vessels and to discriminate between neurogenic and vascular lesions.
- Angiography findings may be diagnostic of neurogenic lesions.
- Carotid body tumors are commonly located at the bifurcation and cause splaying of the carotid bifurcation called the LYRE sign.
- In glomus Vagale, the vagus nerve lies laterally and posteriorly to the carotid system, so these tumors appear as vascular lesions displacing the internal carotid artery (ICA) and external carotid artery (ECA) anteromedially.
Balloon Occlusion Test
- It involves occlusion of the ICA to determine the effect on cerebral blood flow and the adequacy of the contralateral blood flow.
- It is an interventional angiography procedure where there is temporary blocking of the blood flow to the carotid artery. In normal circumstances, the collateral side blood circulation takes over, confirming pre-surgically that the patient will not suffer from fatality related to cerebral stroke.
- It is very critical to prevent any damage to the carotid because if the collateral blood flow does not take over, it can lead to fatality.
- This test poses a risk of neurological sequalae in 4% of the patients.
- This test should be performed when imaging studies suggest carotid involvement or when resection of the lesion carries a high risk of intraoperative carotid artery injury.
Fine Needle Aspiration Cytology
- FNAC is helpful in certain cases, such as neck or oropharynx lumps. It can be ultrasound or CT-guided.
- In carotid body tumors, aspiration of large volume of blood may interfere with cytology. However, such tumors are often fibrous and, therefore, can yield usable suitable cytological material. So, it is better to perform a CT-guided biopsy.
Other Tests
- Metastatic workup: To confirm a suspected metastatic lesion, the primary tumor should undergo a full clinical evaluation, pan endoscopy, and full metastatic workup as directed by the clinical examination findings.
- Positron Emission Tomography (PET) scan: It can be performed to evaluate systemic metastasis.
It is highly recommended that you watch the video lecture on ‘Parapharyngeal Space Tumors’ along with this blog to get a deeper understanding of the topic. In the video, the staging of the Parapharyngeal Space Tumors and approaches to them are also discussed in length.
Treatment of the Parapharyngeal Space Tumors
- The major approach is the complete surgical excision and is recommended for both diagnostic and therapeutic approaches.
- The surgical approach will depend on the following:
- Tumor size
- Location of the tumor (post-styloid or pre-styloid)
- Relationship to great vessels (carotid sheath)
- Malignancy suspicion
- The nonsurgical approach is indicated in the following cases:
- Poor surgical candidates due to tumors of the Co-morbidities
- Elder patients
- Patients in whom balloon occlusion test failed.
- In cases of unresectable lesions (tumors extending to the cranium, retropharyngeal space, etc.)
- The presence of benign, slow-growing tumors would carry a significant risk of sacrifice of multiple cranial nerves.
Radiotherapy for the Parapharyngeal Space Tumors
- If the nasopharyngeal carcinoma is extended in PPS, radiotherapy is the first choice of treatment. Both the primary tumor and the regional nodal metastases are sensitive to radiotherapy.
- It is affected in controlling the growth of carotid body paragangliomas, especially in older patients and patients with co-morbidities.
- It can be used as an adjuvant modality in new cases of deep lobe parotid tumors, even though the recurrence rate is small, mainly because of anatomical considerations.
Chemotherapy for the Parapharyngeal Space Tumors
- Chemotherapy is primarily used to treat rhabdomyosarcomas and other sarcomas of the PPS.
- It can also be used to treat nasopharyngeal carcinomas extending into the PPS. Chemoradiation involves cisplatin and 5-fluorouracil.
- For primary PPS malignancy, chemotherapy should include:
- Doxorubicin for glandular neoplasms
- Cisplatin and 5-fluorouracil for squamous cell carcinomas.
Complications Of the Treatment of the Parapharyngeal Space Tumors
- Bleeding
- Hematoma
- Injury to Facial Nerve
- CSF leaks
- Meningitis
- Injury to Lingual and Hypoglossal Nerves
- Injury to CN IX, X, XI, XII, and cervical sympathetic chain
- Horner's Syndrome
Prognosis of the Parapharyngeal Space Tumors
- Most tumors are benign in nature; thus, five-year survival is > 80%.
- Paragangliomas can be malignant, but the diagnosis needs to be made on the basis of surgical procedures.
- There is relatively good survival for the malignant PPS lesions.
- If the malignant tumors of adjacent spaces have spread to the PPS, the survival is < 10% over 5 years, indicating that PPS involvement of adjacent tumors may cause relative incurability.
Frequently asked questions
Q: What is the most common parapharyngeal tumor?
Answer: Neurogenic lesions
Q: What are the symptoms of the parapharyngeal tumor?
Answer: The main symptoms are:
- Neck swelling
- Oropharyngeal mass
- Nasal obstruction
- Eustachian tube obstruction
- Dysphagia
- Dyspnea due to narrowed oropharynx.
- Dysphonia
- Obstructive sleep apnea
Q: What is the Prognosis of the Parapharyngeal Space Tumors?
Answer: Most tumors are benign in nature and have a five-year survival rate of more than 80%.
Also Read: Unlocking the world of Hearing Aids
Propel your ENT Residency Preparation! Access conceptual video lectures, QBank, Mock Tests, and premium study resources on the PrepLadder App. Download it today!

PrepLadder
Access all the necessary resources you need to succeed in your competitive exam preparation. Stay informed with the latest news and updates on the upcoming exam, enhance your exam preparation, and transform your dreams into a reality!
Navigate Quickly
Introduction
Types of tumors of PPS
Salivary Gland tumors
Neurogenic Tumors
Paraganglioma
Vagal Paragangliomas
Malignant Paraganglioma
Clinical Features of the Parapharyngeal Space Tumours
Diagnosis of the Parapharyngeal Space Tumors
Imaging:
Fine Needle Aspiration Cytology
Other Tests
Treatment of the Parapharyngeal Space Tumors
Radiotherapy for the Parapharyngeal Space Tumors
Chemotherapy for the Parapharyngeal Space Tumors
Complications Of the Treatment of the Parapharyngeal Space Tumors
Prognosis of the Parapharyngeal Space Tumors
Frequently asked questions
Top searching words
The most popular search terms used by aspirants
- ENT Residency Pharynx
PrepLadder for Residency
Avail 24-Hr Free Trial